According to the Cleveland Clinic, cardiovascular diseases (CDVs) are conditions that affect the heart and blood vessels. Cardiovascular disease can cause other organs and systems to be damaged because of decreased or blocked blood flow. Common causes that can lead to an increased risk of cardiovascular disease include:
So why is this condition category so important to us as coders and clinicians? Cardiovascular diseases such as coronary artery disease, cerebrovascular disease, and peripheral arterial disease are some of the leading causes of illness and death in the United States. Cardiovascular disease accounted for 874,613 deaths in the United States in 2019, and almost half of adults in the U.S. have some form of cardiovascular disease.
Risk Adjustment and Cardiovascular Diseases
The V28 risk adjustment model has drastically reduced the number of codes that risk adjusts. In total, over 2,000 ICD-10-CM codes that were previously carrying an HCC weight will no longer carry any weight at all. Cardiovascular diseases are included, with over 190 codes in this section of the ICD-10 alone no longer mapping to an HCC category. Specificity is more important than ever to the financial health of the Federally Qualified Health Centers, as risk adjustment directly affects benchmark leakage and the bucket of shared savings that can be earned in value-based contracts.
Cardiovascular Coding Tips
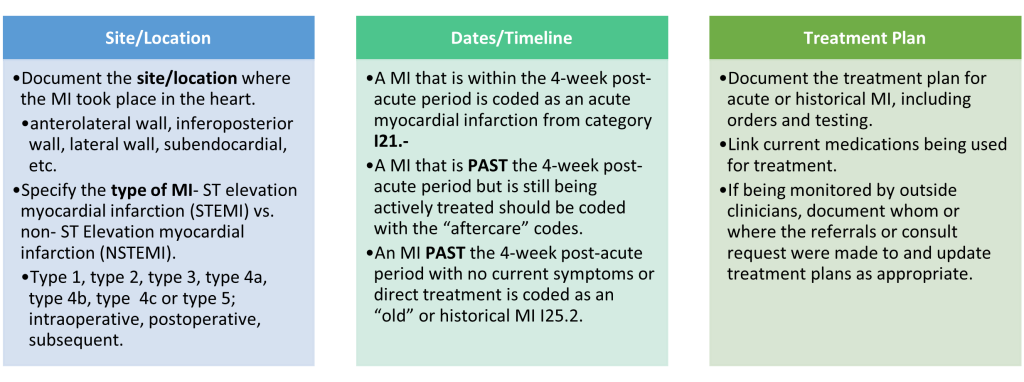
Myocardial Infarction (MI) I21.-
To select the appropriate code, the following should be documented. If unknown, query the provider:
If a type 1 NSTEMI evolves into STEMI, code the STEMI code. Type 1 STEMI can be found in code range I21.0- I21.2, and I21.3 while Type 1 NSTEMI is coded as I21.4. If the myocardial infarction is unspecified, code I21.9 Acute myocardial infarction, unspecified is the default. An MI is PAST the 4-week post-acute period with no current symptoms or direct treatment is coded as an “old” or historical MI I25.2. In the ICD 10 Cm there is a “code also” note to add a code for exposure to tobacco smoke (Z77.2), history of tobacco dependence (Z87.891), tobacco dependence (F17.-), and tobacco use (Z72.0) if present as smoking is an associated risk factor.
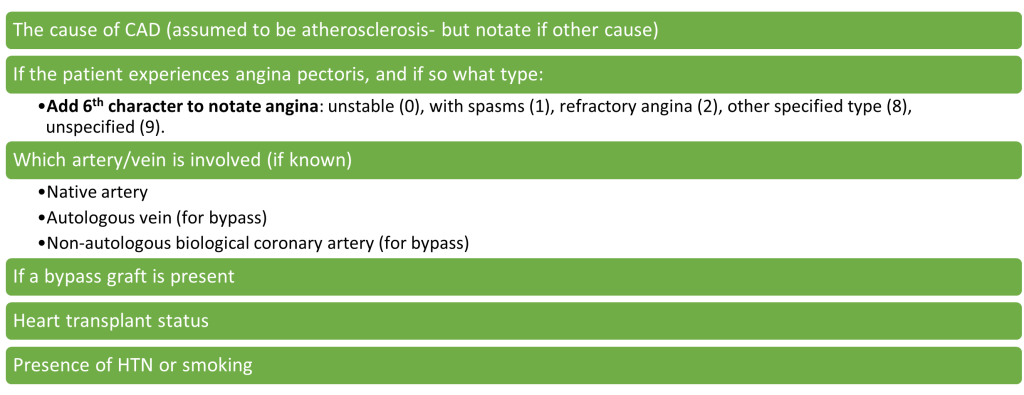
Coronary Artery Disease (CAD) I25.-
There are over 40 codes for atherosclerosis of the coronary artery alone, however most of the codes in this category no longer risk adjust. CAD with unstable angina are the only remaining codes that will risk adjust, totaling up to only eight codes in the category that map to an HCC.
Diagnosis Code
Description
CMS-HCC Model V24
CMS-HCC Model V28
I25.110
Atherosclerotic heart disease of native coronary artery with unstable angina pectoris
87
229
I25.700
Atherosclerosis of coronary artery bypass graft(s), unspecified, with unstable angina pectoris
87
229
I25.710
Atherosclerosis of autologous vein coronary artery bypass graft(s) with unstable angina pectoris
87
229
I25.720
Atherosclerosis of autologous artery coronary artery bypass graft(s) with unstable angina pectoris
87
229
I25.730
Atherosclerosis of non-autologous biological coronary artery bypass graft(s) with unstable angina pectoris
87
229
I25.750
Atherosclerosis of native coronary artery of transplanted heart with unstable angina
87
229
I25.760
Atherosclerosis of bypass graft of coronary artery of transplanted heart with unstable angina
87
229
I25.790
Atherosclerosis of other coronary artery bypass graft(s) with unstable angina pectoris
87
229
To make the proper code selection you will need documentation on:
Cardiomyopathy I42.-
The term “cardiomyopathy” is broad and nonspecific. To code for cardiomyopathy correctly, you will need to know what type the patient has, and the status of the condition as it is currently. The main types of cardiomyopathies are Dilated, Hypertrophic, and Restrictive.
Dilated cardiomyopathy starts in the heart’s main pumping chamber (left ventricle) and makes it harder for the heart to pump blood to the rest of the body. This causes the heart chambers (ventricles) to thin and stretch, growing larger.
Hypertrophic cardiomyopathy occurs when the heart muscle becomes thickened (hypertrophied). The thickened heart muscle can make it harder for the heart to pump blood. Many people don’t realize they have it because they have few, if any, symptoms.
Restrictive cardiomyopathy happens when the muscle tissue in the heart’s lower chambers (ventricles) becomes stiff, and the ventricles can’t fill with blood. This leads to reduced blood flow in the heart.
Documentation should also notate the status of the cardiomyopathy- is it stable, improved, or worsening to support code selection and code validation. If the status of the condition is not specified, or the type of cardiomyopathy is not specific, consider querying the provider for more information. This category of codes will risk adjust, except for cardiomyopathy due to drugs or an external agent (I42.7).
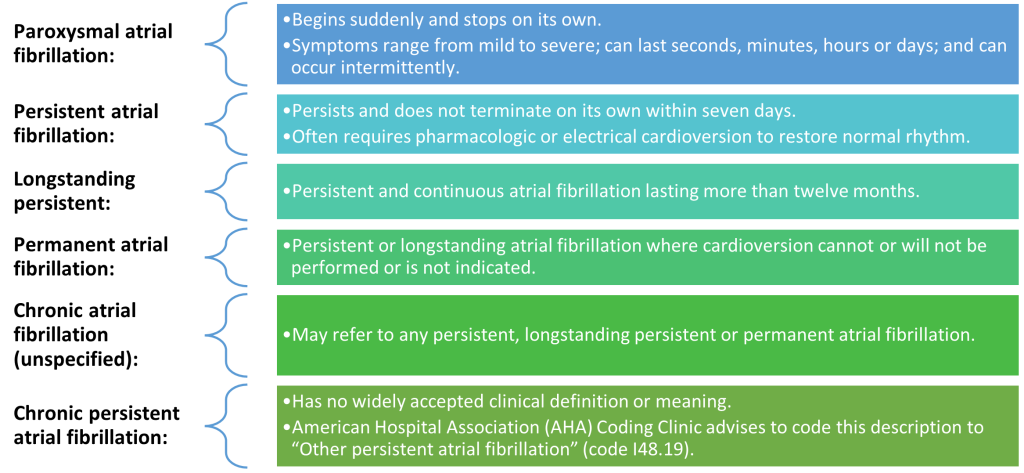
Atrial Fibrillation (Afib) I48.-
This disease category also heavily relies on specificity for appropriate code selection. The elements needed are the type of atrial fibrillation, if the afib is acute or chronic, and if the condition is currently being managed or if it has resolved. If the type of arrythmia is known, do not document and code for non-specific terms like dysrhythmia or arrhythmia.
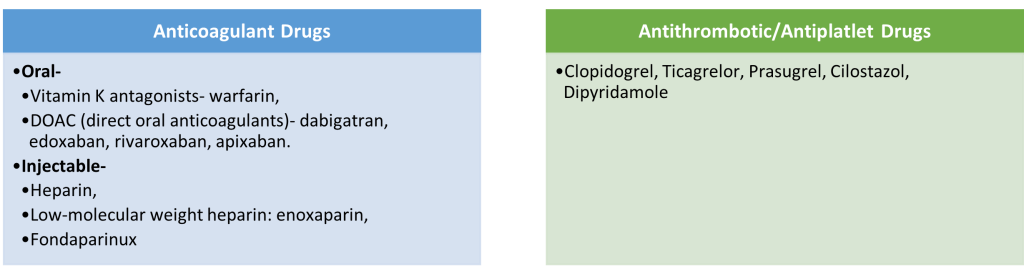
When documenting how the afib is currently being managed and treated, it is important to also link the type of medications used for management if present. Additional codes are needed to describe if the patient is taking an anticoagulant [ Z79.01 Long-term Current Use of Anticoagulants], Aspirin Z79.82 Long term (current) use of aspirin, or antithrombotic or antiplatelet [Z79.02 Long-term Current Use of Antithrombotic/Antiplatelet Drugs] medications.
Some common medications to look out for in the medical record are:
A coder cannot assume anticoagulation therapy is being used to treat atrial fibrillation when there is no documented link between the two in the record. If the link between a medication is not made in the documentation, consider querying the provider for clarification. Code also Z95.0 if a Cardiac Pacemaker is present, or Z95.810 if automatic (implantable) cardiac defibrillator is present. If the afib has resolved and is no longer receiving active treatment or being monitored, code for past medical history of atrial fibrillation (Z86.79).
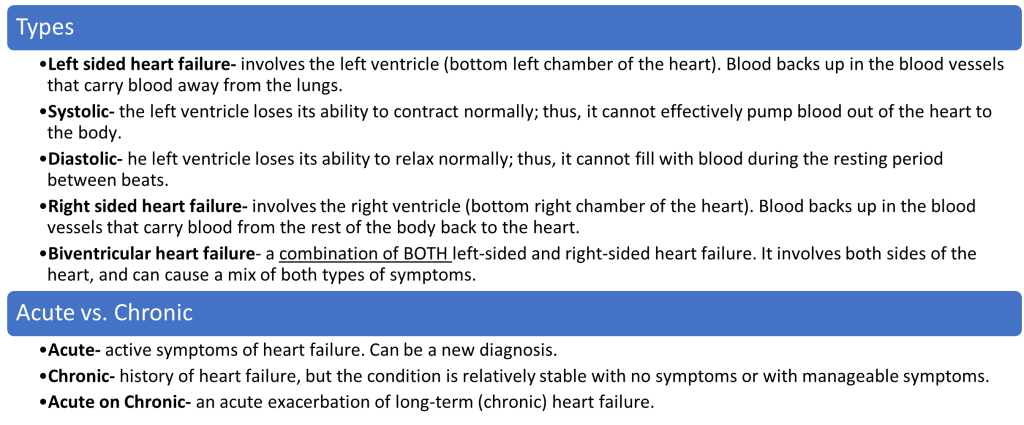
Congestive Heart Failure (CHF) I50.-
To select the appropriate heart failure code, the type of heart failure needs to be known: congestive, hypertensive, postoperative, acute, chronic, acute-on-chronic, diastolic, systolic, etc. If the type of heart failure is not specified, I50.9 for heat failure unspecified is acceptable and risk adjusts but is not recommended if more specificity can be provided. State the cause of heart failure or comorbidities using linking terms to show cause and effect- “associated with,” “due to,” “secondary to,” “hypertensive,” etc. Include the current status of heart failure: stable, worsening, improved, in remission, compensated, decompensated, etc. Do not document “history of” to describe current heart failure. In diagnosis coding, the descriptor “history of” implies the condition occurred in the past and no longer exists.
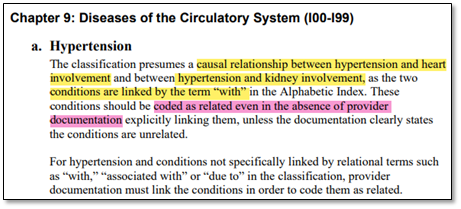
Hypertension coding has an assumed causal correlation with chronic kidney disease (CKD) and congestive heart failure (CHF). Per the ICD-10-CM guidelines, coders have the discretion to code to higher specificity even when not directly correlated in providers’ documentation. This means, if a provider codes I10 for essential hypertension and I50.32 for chronic diastolic (congestive) heart failure on the same date of service, the coder can correct the code selection to reflect I11.0 for hypertensive heart disease with heart failure and include the I50.32 code for the type of heart failure. Always code the CKD code (N18.-) and/or HF code (I50.-) with the hypertension combination code to further specify the type or stage of the comorbidity.
Example:Final diagnosis- Hypertensive heart disease with chronic diastolic CHF and CKD stage 4.
The codes in this category no longer risk adjusts in the V28 CMS risk adjustment model for the most part, with the exception of Raynaud’s syndrome with gangrene (I73.01). This is a heavy hit to clinicians, as a common code used for PVD I73.9 for unspecified PVD no longer will risk adjust. However, if a diabetic patient presents with a comorbidity of peripheral vascular disease, there are combination codes that show PVD as a comorbidity. The HCC this combination code maps to is category 37 for diabetic codes. It will not risk adjust for the vascular disease HCC category like it did in the V24 CMS model when the category was 108.
ICD 10 Code
Code Description
V24 Model
V28 Model
E11.51
Type 2 diabetes mellitus with diabetic peripheral angiopathy without gangrene
18
37
E11.51
Type 2 diabetes mellitus with diabetic peripheral angiopathy without gangrene
108
E11.52
Type 2 diabetes mellitus with diabetic peripheral angiopathy with gangrene
18
37
E11.52
Type 2 diabetes mellitus with diabetic peripheral angiopathy with gangrene
106
263
E11.59
Type 2 diabetes mellitus with other circulatory complications
18
37
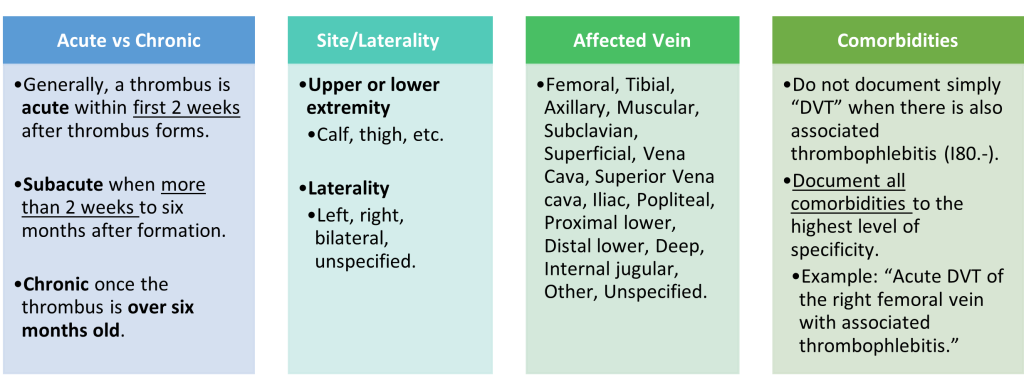
Deep Vein Thrombosis (DVT) I82.-
Deep vein thromboses can happen anywhere in the body, and therefore must have ample documentation on the type (acute vs. chronic), location, laterality, and complications of the thrombosis to select the correct code. Information on when the DVT first occurred should also be clearly documented in the medical record as it also affects code selection on if the condition would be considered acute or chronic.
When a final diagnosis is stated simply as “DVT” but the body of the record documents signs and symptoms that are associated with thrombophlebitis (swelling, erythema, pain and induration), query for clarification and an addendum/correction created when indicated. If the DVT has resolved either through surgery or natural causes, Z86.718 for personal history of venous thrombosis and embolism should be coded in leu of an active DVT diagnosis code. Code also Z79.01 Long-term Current Use of Anticoagulants if the DVT is being managed with. Query the provider when documentation of long-term anticoagulant therapy does not indicate whether this therapy is being used as active treatment of a current DVT vs. historical DVT with for preventing recurrence.